New Zealand’s COVID-19 Containment Strategy and Outcomes
By Srikanta Chatterjee and Nikhil Srivastava
Introduction and objectives
This article examines the experiences of New Zealand (NZ) in containing COVID-19, the viral disease which has been raging around the world since early 2020. After a quick look at selected statistical indicators of NZ’s economy, polity and geography, the article outlines the sequential evolution of the strategy and the policies NZ adopted, their scientific rationale and results. The country’s handling of the deadly contagion has come to be considered globally as being among the few successful ones, to date. The article investigates if NZ offers any lessons which other countries, including India, can make use of and also if NZ itself could have achieved better outcomes.
Pandemic strategy, policy and outcomes
With its population of around 5 million and population-density under 19 persons per square km of its land area, as Table 1 reports, NZ must count as a small and sparsely populated country. Also, the country, made up of a number of islands, is geographically remote from the world’s major population centres. This is helpful in controlling the movement of people, animals or cargo from the rest of the world.
Table 1. New Zealand: Selected Basic Statistics
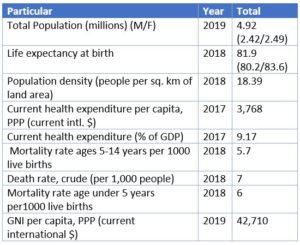
Its per capita income puts NZ in the category of a high-income country. Its life expectancy at birth, crude death rate and the other health statistics, reported in Table 1, indicate that New Zealanders, on average, live a long and relatively healthy life. The country has in place a publicly funded universal healthcare system allowing unfettered access to healthcare, albeit sometimes with a degree of rationing necessitated by the numbers seeking access. Provisions exist for private healthcare too, but its scope is relatively small.
New Zealand recorded its first coronavirus case on 28 February, but its efforts to contain the disease had started earlier than this date and have been proactive and generally well-coordinated. On 24 January, while stating that the risk of the disease was not high, the NZ Ministry of Health put together a team to monitor the developing situation and advise appropriate action. The next day, Australia, NZ’s closest neighbour, reports three cases of the virus. From 27 January, NZ public health officials began meeting passengers arriving at airports from China to monitor early symptoms of the virus. On 30 January, the NZ government repatriated some 200 citizens from Wuhan.
An existing Pandemic Influenza Technical Advisory Group (PITAG) was activated to help improve preparedness for a possible pandemic.
On 3 February, entry restrictions were introduced on non-New Zealanders arriving from, or transiting through, China. Those entering the country were required to self-isolate for 14 days. Anyone arriving from offshore and feeling sick within a month was instructed to seek medical advice. On 29 February, passengers arriving on direct flights from selected east Asian countries were met and checked for symptoms at NZ airports.
By 8 March, several more cases of the disease, all traceable to overseas travel, were reported, indicating the absence of social transmission locally, so far. Even so, a number of planned outdoors gatherings were cancelled. Starting 16 March, with some minor exceptions, everyone arriving in NZ, including NZ citizens, are required to self-isolate for 14 days. Cruise ships were not allowed to dock in NZ ports until 30 June. The Prime Minister (PM) described these measures as being the ‘widest-ranging and toughest border restrictions of any country in the world’, in line with her government’s decision to ‘go early and go hard’. On 18 March, the government urged all New Zealanders travelling overseas to return home. From the next day, all indoor gatherings of more than 100 people, with the exception of workplaces, schools, supermarkets or public transport, were prohibited.
A country-wide four-stage alert-level system was announced on 21 March to deal with the anticipated surge in the spread of the virus; level 1 being the mildest, and level 4 the stiffest. The alert was set at level 2, and people over the age of 70 years and those with a vulnerable immune system are urged to stay at home. The alert level was raised to level 3 on 23 March and all schools are ordered to close starting that day. It was also announced that the alert level would be raised to level 4, two days later, bringing in a nationwide lockdown, with the exception of specified ‘essential services’.
Political parties in the Parliament unanimously passed a nationwide state of emergency on March 25. On that date, NZ has only 205 COVID-19 cases and no deaths. At a later date, the PM revealed that expert advice received in late March had shown NZ to be on a trajectory similar to countries like Italy or Spain, raising the possibility of the case numbers climbing to 10,000 or more by late July, without the strict lockdown.
The gradual and well-publicised advance toward the total lockdown allowed people to prepare better and accept it with greater ease. A team of scientists, epidemiologists and other medical professionals, with the Director-General of Health at the helm, came together to provide necessary help and medical advice to the government. The PM, accompanied by the Health Minister and the Director-General of Health, attended press briefings to explain relevant issues and answer questions regularly. The PM also took to Facebook Live, to ‘check in with everyone’ (in the ‘team of 5 million’ New Zealanders), as the nation locked down.
On 29 March, the NZ police website launched a new online facility for people to report any violation of the rules as prescribed under alert level 4.
In mid-April, the PM and her ministers took a voluntary pay-cut of 20%, in solidarity with the population at large facing financial stringency. The leader of the opposition and the chief medical officer follow suit, accepting a similar pay cut.
The country recorded its first death from the disease on March 29 when a woman in her 70s, who had recently returned from Iran, died. All travels to and from Iran were banned. On 1 April, NZ had 61 new cases, while 82 people have recovered, 14 are in hospital, of who 2 were in the intensive care, but stable. On 2 April, NZ had its biggest single-day increase in case number, with 89 new cases, which brought the total to 797. On 5 April, the total number of cases reached 1039. From April 10, everyone arriving in NZ was required to undergo a 14-day supervised quarantine. Growth in case numbers then started to decline and the alert level dropped to 3 on April 27, after just over a month at level 4. On May 13, NZ moved down to alert level 2. On June 8, there were, again, no active cases within the country, and the PM announced the lowering of the alert level to 1. All restrictions, apart from the border controls, eased and people were permitted to go about life normally.
Some ‘significant clusters’ of cases, defined as situations consisting of at least ten cases which are not part of the same household but connected through transmission of the infection, were identified and controlled to avoid further transmission. All were eliminated by late July.
The relatively small number of locally acquired cases testify to success the strict and early enforcement of social isolation. As Figure 1 records, a large proportion of the cases in NZ have been imported or import-related.
Figure 1. Sources of the COVID-19 Contagion in New Zealand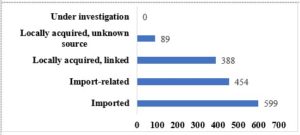
As Figure 2 shows, disease incidence in the 60+ age group, which works out at 19.4% of the total, and is not very large, but when the number of deaths is considered, they are all in this group. This confirms the higher vulnerability of the elderly populations, providing justification for the restrictions advised for those in the 70+ age-group, even at alert level 2.
Figure 2. Age-wise distribution and impact of COVID-19 contagion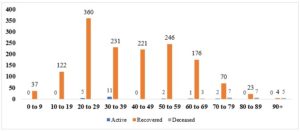
The aim of NZ’s COVID-19 strategy has been not just to contain the virus but eliminate it through a consistent and sustained set of policies, informed by expert scientific advice and sound common sense. The major strands of that policy-setting, as outlined above, included border controls, monitoring the incidence of the disease, physical distancing of people and the observance of some sensible rules of personal hygiene, all clearly communicated to the general public regularly. Surveillance measures put in place include the testing of people with respiratory symptoms and ‘sentinel testing’ in the wider community with a particular emphasis on testing the potentially vulnerable populations even without symptoms of the disease. NZ’s testing capacity of up to 8,000 per day is high, in both absolute and per capita terms. The total testing done between 22 January and 1 August, at over 475,400, ranks among the highest in the world, per capita.
An important part of the strategy of minimising transmission of the virus is the capability to trace contacts of the infected cases and isolate them under supervision within four days of the exposure. NZ’s COVID-19 mitigation plan has been actively pursuing these aims. The Ministry of Health has developed a technology to trace contacts and provide facilities for appropriate quarantining (Q) of actual or potential cases of infection. Facilities for ‘managed isolation’ (MI) of New Zealanders returning home have been created and are being used at public expense. The total number of people who have been through MI and Q from 17 June to 14 August stands at around 19,000, with 98 confirmed cases and 29 active ones.
Despite these notable successes, there have been several deficiencies in NZ’s overall strategy. These include lapses in the residential elderly-care facilities where the casualties have been unduly high. These establishments evidently failed to test residents and staff adequately, train staff appropriately and/or provide personal protective equipment (PPE) on time. These deficiencies have put the entire system of elderly care under public scrutiny and calls are being made to examine the existing infrastructure of elderly care in NZ, identify and rectify its deficiencies.
The number of breaches over the lockdown period from late March to mid-May had been over 2,000, of whom over 200 faced prosecution. Notably, the Minister of Health had breached the rules by driving his family to a nearby beach. The Minister was publicly admonished by the PM but allowed to continue during the lockdown. Once the lockdown ended, the Minister resigned.
In stage 1 of the lockdown, those entering the country are required to spend a specified length of time in facilities with supervised isolation, testing and quarantine arrangements. The management and supervision practices of these facilities have proved to be lax in some areas, resulting in the violation of border control and physical distancing protocols. A senior minister and a high-ranking official of the NZ Airforce have since been brought in to improve administrative discipline and provide expert advice and guidance
With the number of its confirmed and probable cases currently at 1643 – around 328 per million of the population and 22 deaths – NZ’s record of containing COVID-19 is among the successful ones, globally. Its testing record of 47.8 cases out of 1000 is the fifth highest in the world.
Economic impact and response package
While containing the contagion and saving lives has been the primary aim of the government’s emergency policy package, the unavoidably adverse impact of the policies on people’s livelihood also needed to be taken care of. With normal economic and social activities effectively suspended, individuals, families and businesses needed financial support and general help to sustain themselves through the lockdown and the period immediately beyond it. To that end, on 17 March, the government in coordination with the central bank, put together an initial financial package worth NZ$12.1 billion, which is around 4% of its GDP, to cushion the immediate impact. It contained specific financial provisions for businesses and jobs, income support, support for healthcare and for some essential supply chains. A bigger financial package was passed in the Parliament later, with cross-party support, enabling the government to access NZ$52 billion for emergency spending. Several policies have been put in place to alleviate uncertainties and financial hardships to home-owners and renters. An income support package to assist the most vulnerable population and a wage subsidy scheme to guarantee financial help to those thrown out of work because of the lockdown came to be activated. Employers too are being helped to retain employees through the period of the shutdown. Various other sector-specific assistance schemes have been developed to help individuals, families, businesses, social services and charitable organisations.
Side by side with these immediate relief measures, considerations for the period beyond have led to the setting up on 1 April of an Infrastructure Industry Reference Group tasked with identifying useful ‘shovel-ready’ infrastructure projects to be taken up post-COVID. Local governments and various other groups have responded with proposals which can be undertaken promptly to create useful jobs in approved projects. Once the emergency measures stop, further measures would be needed to mitigate the anticipated hardships. Clear indications of these are yet to emerge.
New Zealand entered the lockdown in relatively sound economic health, with a low level of public debt, a steady and sustained, if modest, GDP growth, low and stable inflation, a strong financial system prudentially supervised by the central bank and served by financial institutions and practices which are transparent and generally efficient. These would no doubt help NZ withstand the financial pressures arising out of the relief measures which are funded by public debt. These debts will, of course, need to be serviced and, eventually, repaid, and will entail intergenerational consequences. These issues are well understood by policymakers and the informed public and are already being discussed and debated.
Inevitably, however, the economy will experience significant shrinkage and higher unemployment as a consequence of the lockdown and other restrictive measures. A major aim of the economic relief package has been to inject purchasing power into the economy so that the harm caused by the forced closure of normal activities and the resulting decline in household and business spending is compensated for and the hardship to people’s daily lives mitigated, at least, to some extent.
To summarise, NZ’s policies and practices in combating the contagion throws up several key elements, viz. uniting the nation; empathising with citizens; relying on expert medical and epidemiological advice and input for policy-making; and communicating helpful advice and instructions clearly and transparently with the public. Countries as different as Norway and Sweden in northern Europe, Ethiopia in eastern Africa, China and Taiwan in East Asia and Australia and NZ in Oceania have all dealt with the contagion in their own ways, not always with total or prolonged lockdowns. They have achieved varying results. But their experiences offer some common elements, not dissimilar to those of NZ. Clearly, these elements are all informed by common sense and are therefore useful for policymakers everywhere, albeit with adaptations to suit each country’s political and social culture and institutions.
Incidence of COVID-19 in India and policy response
India currently ranks third in terms of the number of recorded cases, behind the USA and Brazil. Its number of daily infections has come to exceed the USA’s. While the recovery rate has improved to 69% and the case fatality rate is still relatively low, the disease incidence has remained on a rising trend and probably not peaked yet.
So, where has the Indian response to contain the virus gone wrong?
To address this question, one needs to go beyond the issues around the current pandemic and look at some wider but related factual and institutional matters. The most important of these, concern the arrangements and the budgetary provisions India has in place for meeting the healthcare needs – and indeed a few other ‘basic needs’ of its citizens after seven decades of independence. While India’s unique experiment in creating a democratic governmental structure and maintaining it over seven decades may be worthy of admiration, its failure to provide even the most basic civic amenities like health, sanitation, education, security and also human dignity must count among its serious deficiencies. India’s total healthcare spending of 3.6% of GDP, and the public sector’s share in it of a paltry 1.6%, shows up the stark reality that reliable healthcare has remained beyond the reach of the vast majority of the population. There is no dearth of medical expertise in India, but much of it operates in the private sector, while the public sector healthcare facilities, including hospitals, lack even the basic sanitation, hygiene and other infrastructure. It is ironic that, while India has emerged as a favourite medical tourism destination for wealthy foreigners, expert medical care remains beyond the reach of most Indians. Those who can afford it, source their own healthcare needs from the private sector and, even there, malpractices and highhandedness abound, as every Indian knows and dreads, but suffers in silence. It is against this background that one has to understand why in India a pandemic like the COVID-19 becomes a catastrophe almost beyond control.
These shortcomings are exacerbated by the fact that politics in India has become increasingly divided and adversarial, both at the Centre and in the States and often between the Centre and the States. This engenders mutual mistrust and stymies the building of political consensus necessary to unite the country generally and, especially, in times of national emergencies such as the current pandemic.
As I write this, on the 73rd anniversary day of India’s independence, Jawaharlal Nehru’s speech heralding India’s political freedom comes to mind. On behalf of India’s political leadership, Nehru stressed the urgency for independent India to take steps to ‘fight poverty, ignorance and disease … and create … institutions which will ensure justice and fulness of life for every man and woman…’. It is a sad fact that these noble pledges have remained largely unfulfilled.
In a large and densely populated country of linguistic, religious, social and cultural diversity and widespread poverty, policy-setting needs particularly to be transparent and carefully targeted. And, for people to accept policies and offer compliance, a degree of trust in the government and the institutions is called for. Such trust is born out of the people’s perception of the political leadership and their own daily experience of dealing with the public institutions such as the police, the judiciary, the medical establishment and the local, state or the central government agencies generally. It would be fair to say that such trust has increasingly thinned in India. To deal successfully with a national emergency, the primary consideration of a government must be to protect the lives and livelihoods of its citizens, in particular, the most vulnerable of them. The declaration of the COVID-19 related lockdown at four hours’ notice which put the safety, security and the livelihoods of millions of the poorest Indians into chaos is an example of the distance between the ruler and the ruled in India. There is no evidence that the central government had held any dialogue with the other parties in parliament or with any of the state governments to seek to alert and unify the country in its response to the anticipated arrival of the virus.
The economic consequences and social disruption of this single act, which the Prime Minister later apologised for, are likely to prove more devastating and longer-lasting than even the pandemic. Even before the onset of the pandemic, Indian economy had been slowing – the level of employment actually declining over several years and the banking and financial sector, faced with several large defaults by prominent businesses with political connections, needing large capital injections to stay afloat. These problems will now prove even more difficult to address. Interestingly, much of the government’s supposedly large pandemic relief package has been aimed at boosting the capital shortfall of the financial sector.
Political leaders and high-ranking officials in India have come to form a distinct class of their own, demanding and often receiving unquestioned public adulation and bestowing, in return, ‘gifts’ to the faithful, at public expense, and punishment to those who question them. Public accountability is not an important part of independent India’s political culture, nor is the right to oppose or criticise considered necessary for a healthy democracy. Policymaking, as a consequence, is often arbitrary and ill-considered. Yet, it should not be impossible for the elected representatives in the world’s largest democracy to set aside their ideological differences and cooperate in the decision-making processes for the benefit of their constituents. India’s bureaucratic establishment is made up of highly qualified and well-trained personnel. It is for the political leadership to take them into confidence in seeking to formulate policies.
To finish with a story about a Prime Minister (PM) of another established democracy which had just achieved some relief from its strict lockdown and people were starting to enjoy a more normal life. On a Saturday morning stroll, the PM of the country chanced upon a café hosting its customers. Wishing to join them over brunch, the PM approached the café owner who recognised the PM but declined a seat because that would not fit in with the distancing rule still in force. The PM accepts it and walks on. Happily, however, the PM is called back soon enough as seats become available.
The PM and the country must remain nameless, but the apparently apocryphal story is not so. And the democratic culture reflected in the incident is exemplary and inspiring.
Postscript
As I complete writing this article, NZ, after 102 days without any local transmission, is reporting several new cases of the virus, all confined to one geographic area of the country. The process of tracing and isolating cases started immediately. Testing of people with symptoms, already high, is ramped up and others without symptoms are tested at several places to minimise the spread of the virus. Alert level 3 has been introduced in the area affected and alert level 2 in the rest of the country. Starting with four new cases, the number has risen to 13 confirmed cases after seven days, and all but one of these cases are connected to the same source. How it all pans out remains to be seen.
AUTHORS
Srikanta Chatterjee, Emeritus Professor, School of Economics and Finance, Massey University, New Zealand
Nikhil Srivastava, doctoral candidate, School of Economics and Finance, Massey University, New Zealand
Disclaimer: The views and opinions expressed in this article are those of the author/s and do not necessarily reflect the official policy or position of Azim Premji University or Foundation.
